Feature Article, October 2000
This month's feature article comes from Brandon Bertolli, a Radiographer at the Johannesburg Hospital Adult
Trauma Unit, Johannesburg, South Africa. Mr. Bertolli has provided some insight into the day-to-day operations of the
hospital and has added some interesting gunshot case profiles.
Adult Trauma Unit
Johannesburg, South Africa
In 1999 the Johannesburg Hospital Adult Trauma Unit processed 16325 patients in total. Just over 8000 of
those were due to violent assault, of which 1755 were gunshot victims. Just under 8000 of the total patients had suffered some
kind of accident, whether it was traffic, domestic, or work-related. The rest of them (a small percentage) were sports
injuries or other injuries which had a questionable cause, such as pathological fractures. Of the total patient load, 10% of
patients were injured severely enough to be resuscitated. There was an 88% success rate for resuscitated cases. There
were 45 patients brought to hospital who were pronounced dead on arrival.
There were multiple incidents of staff being threatened with violence by patients or patients relatives, and I
often removed firearms from patients prior to X-Raying them. The hospital security staff were unarmed except for batons, and they
had no bullet-proof vests. Thus we initially relied on the Flying Squad to help us out when people got out of hand.
Unfortunately, a number of incidents occurred which forced many doctors (and a few Radiographers) to come to work armed :
- An ENT specialist was shot dead at the hospital gates by four youths, the oldest of which was 18.
- A nurse was thrown out of her own 6th floor window in the nurses residence.
- Another nurse was shot dead in her 12th floor flat, in the doctor's/nurse's residence, in the same residence block that I was
living in.
- Another nurse was stabbed in the head in the other residence block.
- An AK-47 assault rifle was found under some bushes on hospital premises.
- A doctor was threatened by an armed patient, who demanded he remove a bullet from his foot, or he would shoot the doctor. The
patient had already had the appropriate treatment from the orthopedic surgeons.
- There were increased threats to shoot Trauma Unit doctors. At least three doctors were hijacked and assaulted, while still
wearing their doctors uniforms.
Many of us went for handgun training with the Flying Squad and we were trained to intermediate level. Many of
the doctors were reserve policemen as well. It is not uncommon for the doctors to have firearms concealed under their trauma
clothing. Of course, this is not supported by the hospital management, but security did not remove the guns from us, because they
knew that if there was a problem, they were unarmed themselves, and they would have to rely on us.
Glaser Safety Slug Wound
I X-Rayed this guy while I was on night duty in Johannesburg. He couldn't tell us who shot him, or at what range he was
shot.

The copper cup on X-Ray is the tell-tale Glazer (or variant) sign. The patient lost substantial
amount of Triceps muscle in theatre because it was necrosed.

He also caught a few fragments in his chest wall (see the X-Rays) but they didn't penetrate
deeply enough to cause him a haemothorax or pneumothorax.

FMJ Bullet Through Spine
Another night duty patient from our Johannesburg trauma unit...
This guy was shot with a FMJ bullet, somewhere around 9mm caliber (you can't use X-Rays to
measure exactly, because of magnification). The entrance wound is anterior and the paper clip entrance marker isn't obvious on this
picture, so I've circled it.

The bullet fractured L4 (Fourth Lumbar Vertebra) and drove fragments of bone into the spinal
canal, before finishing up posteriorly. See X-Rays and CT scan.
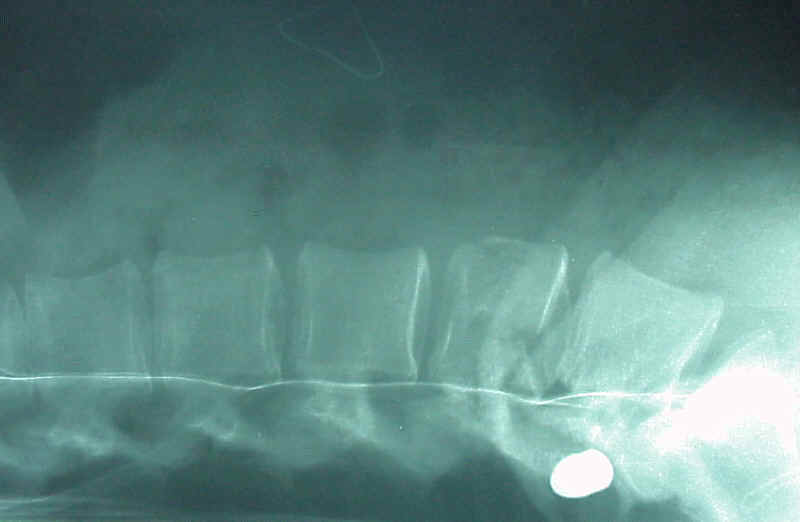

Fortunately the spinal cord doesn't go all the way down to L4, so he had minimal neuro-deficit.
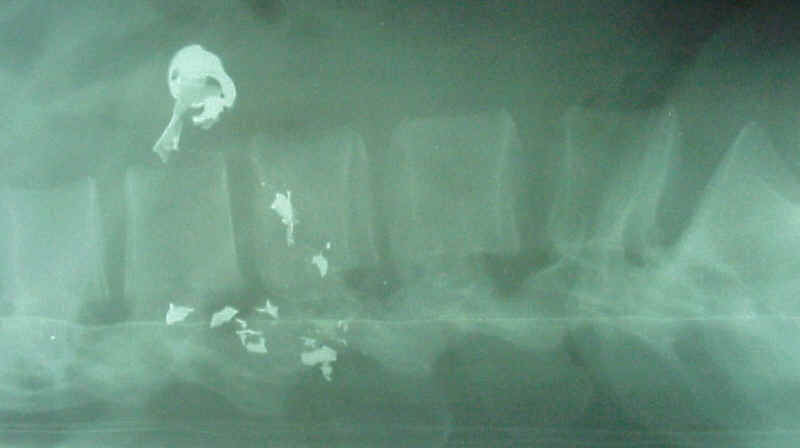
SJHP Bullet Through Spine
Yet another night duty patient from our Johannesburg trauma unit...
This guy was shot with a bullet which was not completely jacketed, probably a SJHP somewhere
around 9mm caliber (you can't use X-Rays to measure exactly, because of magnification). The entrance wound is posterior, marked by
the paper clip triangle. The bullet fractured L2 (2nd Lumbar Vertebra) and pieces of the jacket were shed off into the spinal canal
and around the vertebra. Its unlikely that a FMJ would give these appearances (there was nothing remarkable about the entrance
wound.) See X-Rays and CT scan.
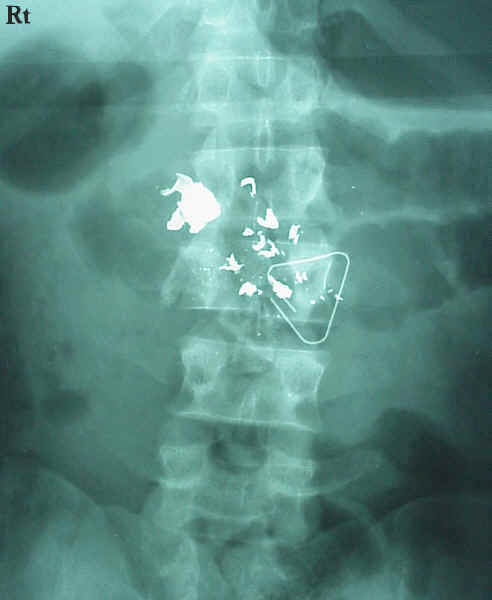
Unfortunately the spinal cord can be damaged at the level of L2, and this patient had definite
neuro-deficit (loss of power and sensation in the legs, worse on the right.) Note that the jacketing appears less dense on X-Ray
than the lead core.
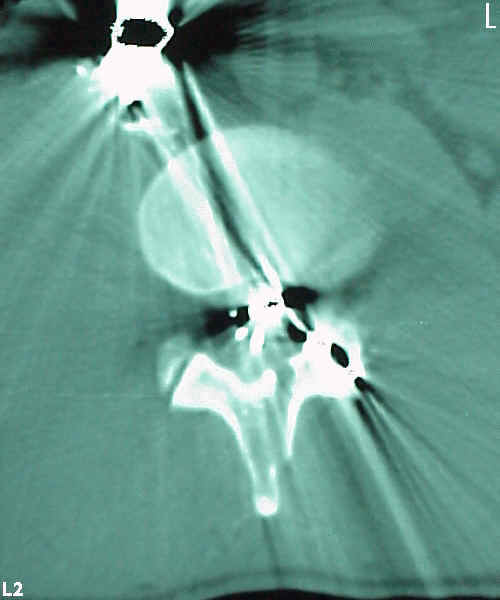
Both of these cause obvious technical artifacts (streaking) on CT scan images.
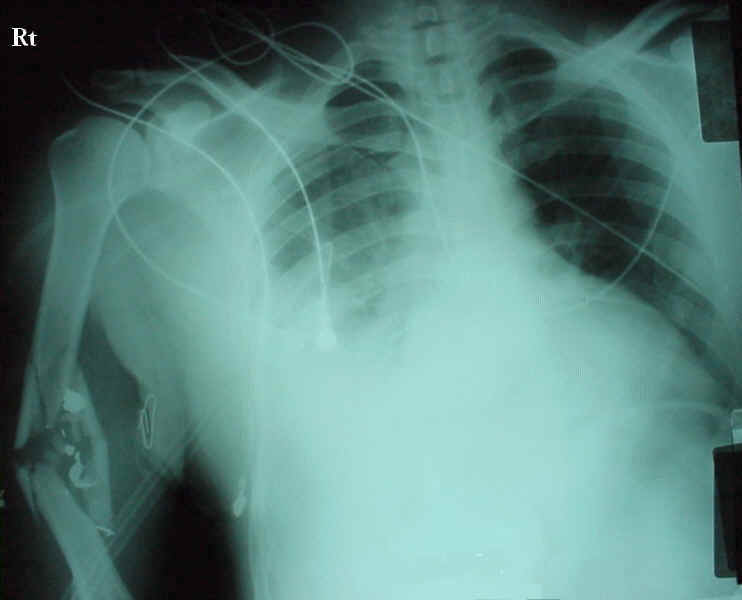
Gunshot Chest and Arm
This guy was one of the 1755 gunshot victims seen by us at the Johannesburg Hospital in 1999.
The bullet entered the right anterior chest, perforated the lung and exited through the right
lateral chest wall and re-entered the right upper arm, fracturing the right humerus. The patient suffered a right haemo-pneumothorax,
but was okay after treatment. The X-Ray is an AP seated chest view.
If anyone has any questions about X-Rays or anything really, you can contact me at bbertolli@yahoo.com.
All images seen on this page are copyright © 2000 Brandon
Bertolli. All rights reserved.
|