Feature Article, April 2002
This month's feature article comes from Brandon Bertolli,
who is researching gunshot wounds in South Africa. Most of
this research will be conducted in the adult trauma unit of the
Johannesburg Hospital, Johannesburg, South Africa. This is Mr. Bertolli's second
submission and I would like to thank him for taking the time to
submit these interesting case studies to firearmsID.com!
Adult Trauma
Unit-Case Studies
Johannesburg, South Africa
The following gunshot injuries were encountered
by Brandon Bertolli in 1999 at the Johannesburg Hospital in South
Africa. They are examples of unexpected X-ray findings, or
findings which did not match the clinical picture.
A 35 year old man was carjacked and
forced to ride along with his assailants. He was beaten, shot
twice then thrown out of the moving vehicle on to the highway. He
was brought to hospital with a gunshot wound to the abdomen and to
the leg. His condition was critical. A supine abdominal X-ray was
done in the resuscitation bay:

The abdominal wound was a very small hole on the
anterior left side of the abdomen, marked with a paperclip. A
small bullet can be seen in the pelvis. It is typical of a bullet
to "point" to the entrance wound, provided it has not been
deflected or deformed. This happens because the bullet's centre of
gravity is towards its base, and it may tumble base-first as soon
as it loses its gyroscopic stability which it gained from the
rifling of the barrel.
The patient's blood pressure could not be
stabilized and despite every effort, he died. We were all very
surprised that this little bullet had penetrated so deeply,
obviously rupturing a major blood vessel.
I later placed one of my .25 cartridges over the
bullet shadow on the film and the bullet in my cartridge matched
the outline of the bullet on film exactly. This does not prove
that a .25 was used, but indicates that no caliber larger than .25
was used. We cannot use X-rays to measure caliber precisely
because all X-ray images are magnified to some degree. However, we
can exclude calibers in situations such as this. The bullet shadow
on X-ray film represents the largest caliber that the bullet can
possibly be.
A young man sustained a gunshot wound to the
left foot. There was a single skin breach over the first
metatarsal, but no other breach could be found. As part of the
standard projectile tracking protocol, a paperclip was taped to
the patient's foot to mark the skin breach for X-ray. Here's what
we found on the first view, the AP:

The first metatarsal is fractured and the
paperclip overlies the fracture. No obvious metallic density can
be seen in the vicinity of the fracture and no bullet can be seen
on this view. So where did the bullet go? The lateral view of the
foot reveals the bullet:

The paperclip fell off before the X-ray was
taken, so I've marked where the skin breach was (E). The bullet
entered the foot dorsally, fractured the first metatarsal then
veered posterior and lodged beneath the heel. This demonstrates
how bullets need not follow a straight path, especially after
hitting bone.
An infant, around two years of age, was brought
to hospital by his parents who claimed he had been struck by a
stray bullet that had entered their apartment through a window.
Upon removing his nappy (diaper) prior to X-ray, I found a loose
fired FMJ bullet and a small breach in the skin on the right hip.
I assumed that the bullet that I found in the nappy was the same
bullet that had given the child the small skin beach. I now had to
weigh up all the options. You must have good reason to X-ray a
child's pelvis, as the young reproductive organs are especially
prone to damage from ionizing radiation (X-rays).
I reasoned that there was the slight possibility
that the bullet had penetrated deeply enough to cause a bone
injury, then bounced back out of the wound. I also had to take in
to account the extra variable of the elasticized nappy. I decided
to do the X-ray, but remembered not to use a lead shield over the
gonads since this was a gunshot pelvis and you should not use lead
for that, since it may hide a bullet. Imagine my surprise when I
saw this film:

A second bullet! Before doing another view
(extra radiation) I checked the child's perineal area and crease
of the buttocks for another loose bullet, but found nothing. I did
this lateral (side) view of the pelvis to localize the bullet:

These two views proved that the bullet was
lodged in the child's scrotum. I was puzzled by the bullet that I
had found lying loose in the nappy - how did it get there? There
was only one skin wound on the child. When I asked the parents how
many shots they had heard, they became curt and unhelpful. I did
not press the matter, just reported my findings to the casualty
doctor. He should have found the loose bullet when he examined the
child. This case proves that an entrance wound need not be the
same size as the bullet, and one cannot assume that a recovered
bullet belongs to a particular wound, without X-ray confirmation.
It also underlines the rule that no gonad shielding must be used
in gunshot wounds of the pelvis. If I had used lead shielding, I
would have missed the bullet.
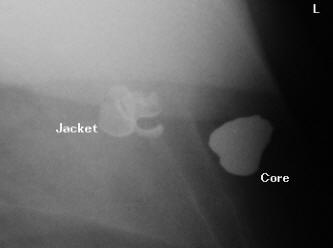
An obese man was shot in the chest by a
carjacker. Upon arrival at hospital, the patient was stable and
fully co-operative. An AP erect chest film was obtained:

Two metallic bodies can be seen, of two
different densities. The person who X-rayed this man did not use
paperclips, and when I went to speak to the patient, he had a very
large dressing on the right side of his chest. Unfortunately I
could not see where the entrance wound was. Nevertheless the
evidence is plain to see. This is a core-jacket separation. A
novice hospital worker may mistake it for two separate
projectiles. The jacket appears as a less dense, sharp-edged
folded density while the core, being lead, is very dense and less
likely to form sharp edges and angles even if it is deformed.
The patient was fit enough to stand for a
lateral view of the chest. Here is a magnified portion of that
view:
Note the difference in densities between the
core and the jacket. Usually the core will penetrate the target
more deeply than the jacket. A special consideration in South
Africa, with the high incidence of HIV infection in the
population, is the risk of being cut by a detached jacket in
surgery. The surgeon needs to be especially careful with jackets
in the operating field. If a surgeon can retrieve the jacket for
forensic analysis, he should use plastic forceps to prevent adding
tool marks to the evidence.
A middle-aged man was sitting in a parked truck
with the engine turned off. A carjacker appeared at the side
window and ordered the man out. The man refused to get out and
instead started the engine, whereupon the gunman immediately
opened fire. Because the vehicle was a truck, the victim was
sitting higher than the level of the hijacker's head. So the
gunman had to aim up if he wanted to shoot the victim in the head.
Fortunately for the victim, the gunman was not accurate and hit
him in the right acromion (shoulder) area. Perhaps the error of
parallax played a role here, too. The bullet was deflected up from
the shoulder into the frontal sinus region of the head; more
specifically just lateral to the frontal sinus. The hijacker fled
without firing any more shots.
The victim arrived at the hospital fully co-operative and stable.
The bullet was palpable under the patient's skin
and it was decided to do skull X-rays to determine its exact
location. The reason was that if he did not have a fracture and if
his frontal sinus was not involved, then he could be kept for
observation and avoid having a CT scan of his brain.These are the views, which were obtained:


Cars are right-hand drive in South Africa. The
victim was facing the gunman at the time of the shooting, looking
at him over his right shoulder. This explains how he sustained
this unusual wound. On X-ray you can see that all the opacities
are of the same density and that there are metallic specks near
the bullet. If you look at the bullet outline carefully on the
lateral view you'll notice that it fits the semi-wadcutter
profile.
The films were shown to the neurosurgeon. He was
not happy with the position of the bullet, since it could not be
proven whether it had breached the sinus or not. A CT scan was
ordered:
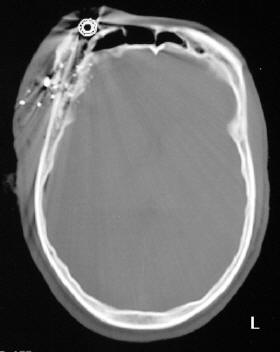
On this bone window slice you can see that the
bullet has caused a frontal bone fracture and there is now a wound
channel from the skin to the frontal sinus. This represents a
significant infection risk. The decision was taken to debride the
wound and keep the patient in for observation and make sure he did
not develop an infection. Note that the CT scan gives the false
impression that the bullet is a hollow point. This is an artifact.
The bullet was solid lead. No intracranial
hematomas were demonstrated on the brain
window slices.
The patient's shoulder was X-rayed but nothing
unusual was discovered. We could not find any other metallic
densities in his clothing. The bullet was definitely all-lead.
Considering it is an all-lead semi-wadcutter, it is most probably
a bullet fired from a revolver.
The patient made a full recovery.

If anyone has
any questions about X-Rays or raytracing (or anything really), you
can contact me at bbertolli@yahoo.com.
All images
seen on this page are copyright © 2002 Brandon Bertolli.
All rights reserved.
|